The Regenerative Potential Of Blood
Derived Autologous Matrix - Case Reports
Dr. Paromita Mazumdar1
Dr. Shromi Roy Choudhury 2
Dr. Sampurna Dutta Gupta3
19
The Regenerative Potential Of Blood Derived
Autologous Matrix - Case Reports
ABSTRACT
The concept of regenerative endodontic procedure have emerged from the field of
tissue engineering which emphasizes the spatial assembly of distinct stem cells,
growth factors/ morphogens, and scaffolds to form a functional tissue or organ.
Cases described in the article illustrate three techniques employed for regenerative
endodontic procedure namely, induction of bleeding into the canal space,
introduction of biological scaffold into the canal space and a modified technique of
induction of bleeding followed by introduction of biological scaffold for regeneration
of pulp dentin complex. All cases performed are showing favorable treatment
outcomes at and are still under follow up. The use of blood derived autologous
matrix may be may be a treatment option which will reduce the need for store of
materials and equipment at the same time paving the way towards customised
biological alternatives for treatment.
KEYWORDS - Intracanal bleeding, biological scaffold, autologous matrix, regenerative endodontic
procedure
Running Title: Three protocols of regenerative endodontic procedure.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
20
INTRODUCTION
The goal of regenerative dentistry is to induce biologic replacement of dental tissues and their supporting
structures. Regenerative endodontics has been defined as biologically based procedures designed to replace
damaged structures such as dentin, root structures, and cells of pup-dentin complex.1 These concepts have
emerged from the field of tissue engineering which emphasizes the spatial assembly of distinct stem cells,
growth factors / morphogens, and scaffolds to form a functional tissue or organ.
Pioneering work supporting the concept of regenerating dental tissues was reported more than 50 years ago
when Dr. B.W. Herman described the application of calcium hydroxide for vital pulp therapy2, and Professor
Nygaard Ostby evaluated a revascularization method reestablishing a pulp-dentin complex in permanent teeth
with pulpal necrosis.3 Blood Clot (BC) or platelet concentrates have been used as scaffold in regenerative
endodontic treatment (RET). The blood clot formed in most cases have been found to serve as a protein
scaffold, permitting three-dimensional in growth of tissue, thereby fulfilling the goal of regenerative endodontic
procedure. Studies have shown the potential of using platelet concentrates as scaffolding in tissue regeneration.
Platelet concentrates are autologous, reasonably easy to prepare in a dental setting, and comprise high
concentrations of growth factors including transforming growth factor-beta (TGF-beta), vascular endothelial
growth factor (VEGF), and platelet-derived growth factor (PDGF).4 PRF forms an organized fibrin network in
which platelets and leukocytes are trapped. These entrapped cells serve as a reservoir of various growth factors
for long-term release. Important circulating immune cells and various cytokines in PRF clots also act against
infection. CGF (Concentrated growth factors) also plays a similar role in regenerative endodontic procedures.
In addition, the mechanical properties of PRF might facilitate the condensation of overlying MTA. In lieu of
routine endodontic practice this case report has been performed for regeneration of pulpal and periodical tissues
using biological scaffolds/ growth factors/ stem cells, calcium hydroxide, mineral trioxide aggregate,
biodentine. The following cases have been performed and documented following the CARE case report
guidelines (2013). 5
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
21
CASE REPORTS
The clinical procedures described in the article have been registered with the Clinical Trials Registry-India
[CTRI number- CTRI/2020/01/022892] and duly approved by the Institutional ethics committee. All the cases
were performed on healthy individuals without contributory medical history. All the participants were
explained the treatment plan and informed consent were obtained.
Three protocols were followed in the cases described below. In the first protocol, bleeding was induced in the
root canal. A biological scaffold (PRF/CGF) was introduced in the canal space in the second protocol without
induction of bleeding. The third protocol was a modified technique where induction of bleeding followed by
introduction of biological scaffold (PRF/CGF) in the canal space was done.
The treatment in all the cases was conducted in two appointments in accordance with the American
Association of Endodontist (AAE) Clinical Considerations for a Regenerative Procedure (Revised 4/1/2018).6
Access cavity preparation was done under local anesthesia under rubber dam isolation in the first appointment.
Cleaning, shaping and copious, gentle irrigation was done with 20ml of 3% NaOCl (20mL/canal, 5 min) using
a 30 gauge side-vented needle. 0.9% normal saline and EDTA (20 mL/canal, 5 min), with irrigating needle
positioned about 1 mm from root end. The canals were dried with paper points, and calcium hydroxide (water-
based) was placed in the canal for a period of seven days. The access cavity was temporarily restored with
Cavit. In the second appointment, on assessing the patient’s response to the initial treatment, if asymptomatic,
the calcium hydroxide was removed with H file and copious saline irrigation under a dental operating
microscope. A final wash of 20ml of 17% EDTA was done. The canals were dried with paper points and
over instrumentation was done in the canal space to cause induction of bleeding. Biodentine/ MTA was then
mixed and plugged till the cementoenamel junction. The access cavity was restored with light cured composite
resin.
In the second protocol, apart from the procedures followed above in the second appointment, if the patient was
asymptomatic, biological scaffold (PRF/CGF) was introduced in the canal space. For preparation of the PRF
membrane, 10 ml of blood was drawn from the patient in two 5 ml syringes (without anticoagulant). The
collected blood was centrifuged at 3000 rpm for 10 minutes. The second layer formed was taken out with help
of a forceps and was placed on a sterile gauge and the excess liquid was squeezed out to obtain the PRF
membrane. The membrane was cut into 1x1mm squares with scissors and plugged into the canal space. The
centrifugation cycle followed for preparation of CGF membrane was 30 seconds acceleration, 2min- 2700
rpm, 4 minutes - 2400 rpm, 3 minutes- 3000 rpm, 36 seconds deceleration. Biodentine/ MTA was then mixed
and plugged till the cementoenamel junction. The access cavity was restored with light cured composite resin.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
22
In the third protocol both induction of bleeding by over instrumentation and introduction of the biological
scaffold (PRF/CGF) into the canal space was done.
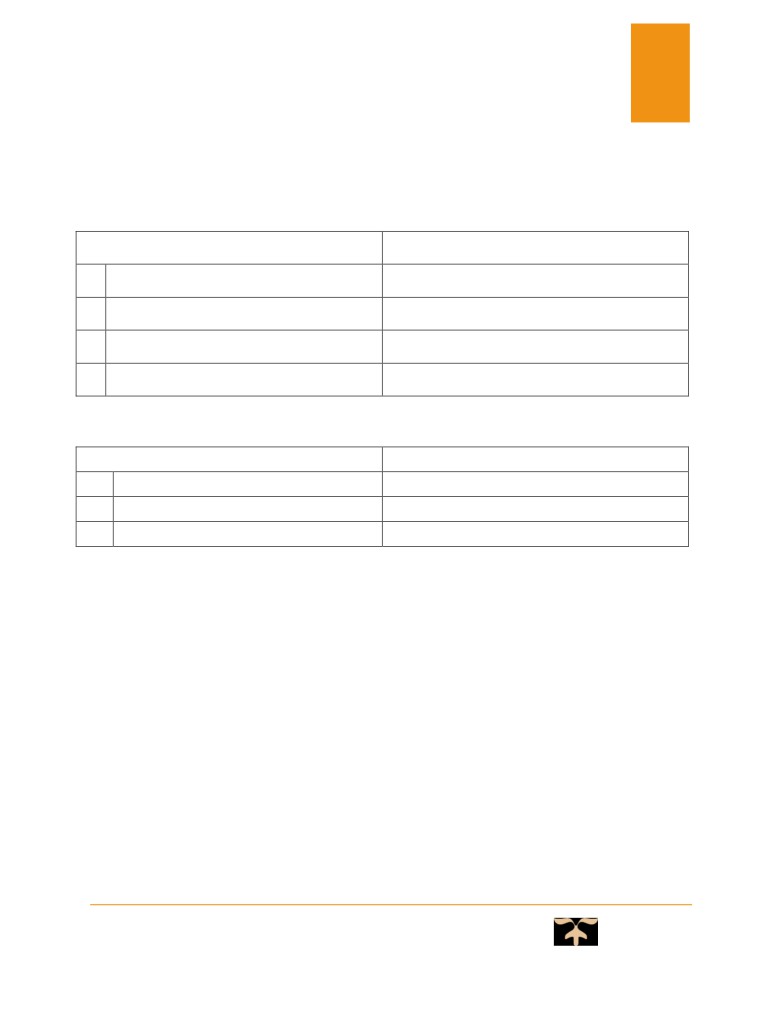
Materials
Manufacturer
1
Mineral tri oxide aggregate
Pyrax Polymars, Lot no: 137553339
2
Biodentine
Septodont,
3
Cavit
3M ESPE
4
Light cured composite resin
Swisstec, Coltene Whaledent
Table 1
Equipment
Manufacturer
1
Centrifuge machine
Remi
2
K files, H files
Dentsply
3
Scissors, Plugger, mirror, tweezers, forceps
GDC
Table 2
Case 1
A thirty two year old male patient reported to the department complaining of pain in the upper front tooth
region. The patient gave history of root canal treatment with the upper front tooth 3 years back. Clinical
examination revealed root canal treatment done with 11 which was tender on vertical percussion. The tooth
responded negatively to pulp sensibility tests (heat test, cold test and electric pulp test). Intra oral periapical
radiograph revealed previous root canal treatment and periapical radiolucency with 11. On the basis of clinical
and radiographic examination, it was diagnosed to be chronic periapical abscess with 11. Considering the
clinical signs and symptoms, regenerative endodontic treatment was planned with 11. In this case first protocol
of inducing of bleeding in the canal space was followed.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
23
Case 2
A 17 year old female patient reported to the department complaining of discoloration in upper front tooth
region since 2 years. . Clinical examination revealed discoloration and Ellis Class III fracture with 21. The
tooth responded negatively to pulp sensibility tests (heat test, cold test and electric pulp test). Intra oral
periapical radiograph revealed radiolucency involving enamel dentin and approaching pulp with 21. On the
basis of clinical and radiographic examination, it was diagnosed to be pulpal necrosis with respect to 21.
Considering the clinical signs and symptoms, regenerative endodontic treatment was planned with 21. In this
case the second protocol of introduction of biological scaffold into the canal space was followed.
Case 3
A thirty seven year old male patient reported to the department complaining of pain in the upper right back
region of the jaw. Clinical examination revealed proximal caries with 14 with a probing depth of 4 mm. The
tooth was tender on vertical percussion. The tooth responded negatively to pulp sensibility tests (heat test, cold
test and electric pulp test). Intra oral periapical radiograph revealed radiolucency involving enamel, dentin and
pulp on the distal aspect of the crown portion of 14 with periapical radiolucency. On the basis of clinical and
radiographic examination, it was diagnosed to be pulpal necrosis with symptomatic apical periodontitis with
14. Considering the clinical signs and symptoms, regenerative endodontic treatment was planned with 14. This
case was performed using the modified technique of induction of bleeding followed by introduction of
biological scaffold into the canal space.
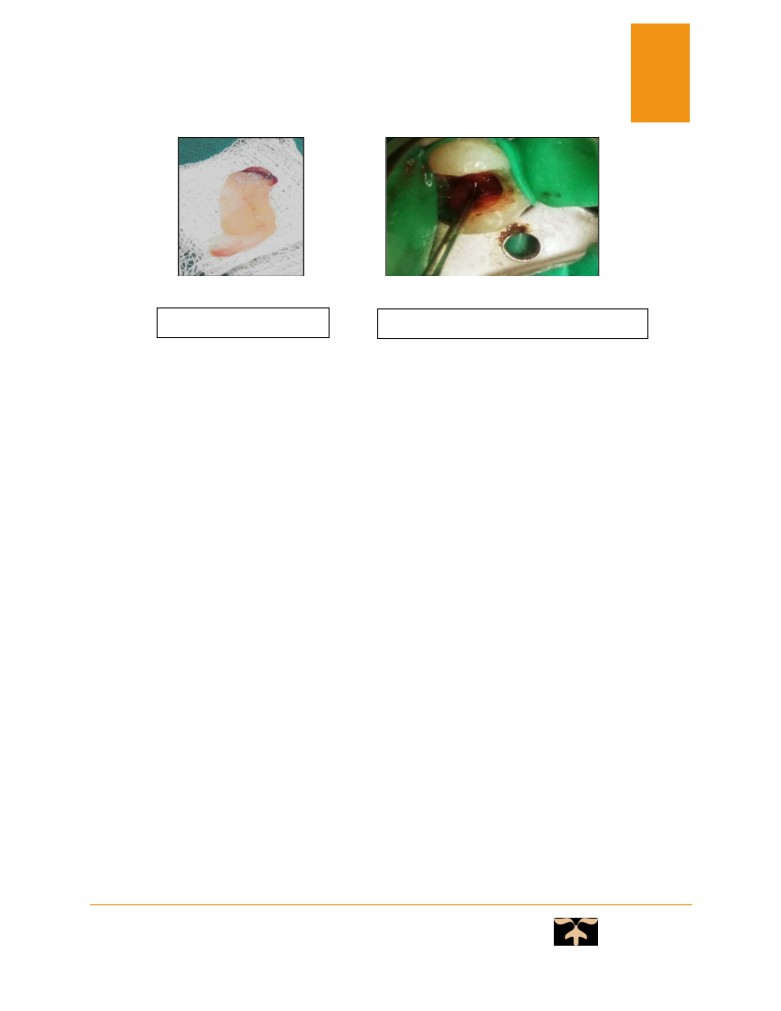
Access opening with 14
Induction of bleeding
Centrifugation
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
24
PRF membrane
Plugging of PRF membrane in canal
space
The patients were asked to report to the department in event of any untoward circumstances with the treated
tooth.
The patients were recalled for follow ups at an interval of 1 month, 3 months, 6 months and 1 year. Pulp
sensibility and vitality test was performed after 6 months.
Follow Up
The patients were followed up on basis of clinical and radiographic criteria. Clinical criteria consisted of the
following:
•
Pain
•
Pain on palpation
•
Presence/absence of swelling
•
Presence/absence of mobility
•
Tenderness on percussion
•
Presence/absence/ healed intraoral swelling/sinus
The radiographic criteria were:
•
Healing of preexisting bony periapical lesion
•
Increase of root thickness and length
•
Absence of (continuous) external root resorption
•
Radiographic detection of a new PDL along the inner wall of the root canal.
Radiographic assessment was done on the basis of periapical index score given by Orstavik et al in 1986.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
25
The follow up is listed in the tables below:
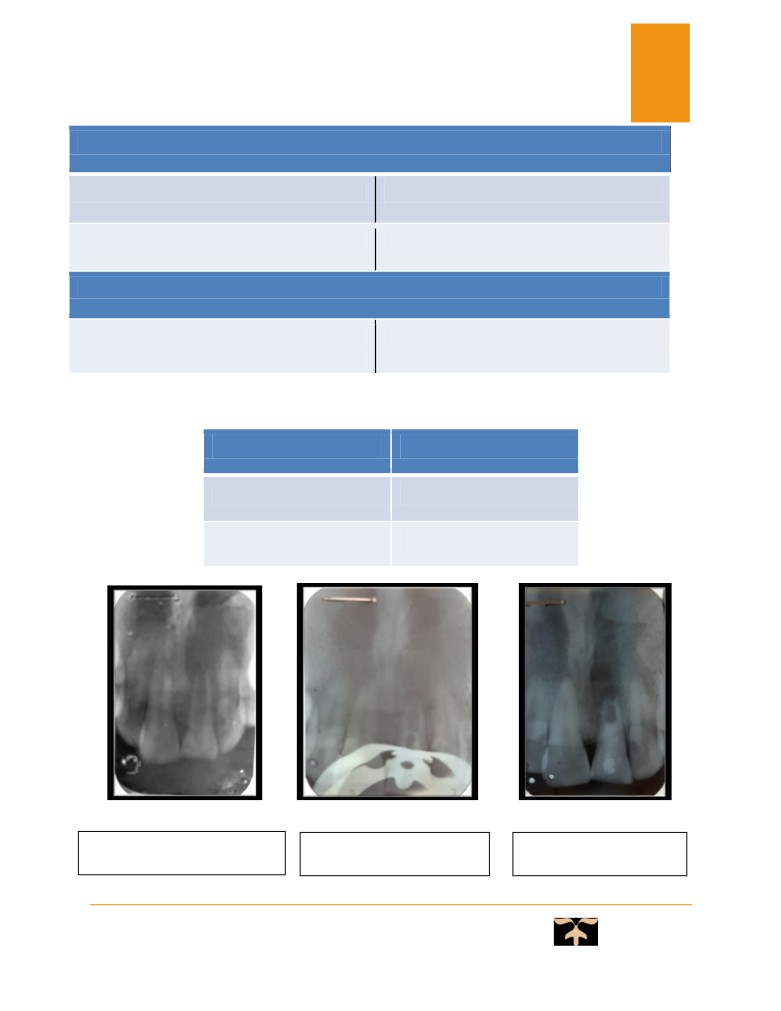
Case 1
Follow up
PAI score
1 month
4
3 months
2
6 months
2
Pre operative IOPA-R with 11
After 3 months follow up
After 6 months follow up
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
26
PULP SENSIBILITY TEST
THERMAL (COLD)
Delayed response
ELECTRICAL PULP TESTING
Delayed response
PULP VITALITY TESTS
PULSE OXIMETRY
62 (normal range=71%-92.7%)7
(OXYGEN SATURATION)
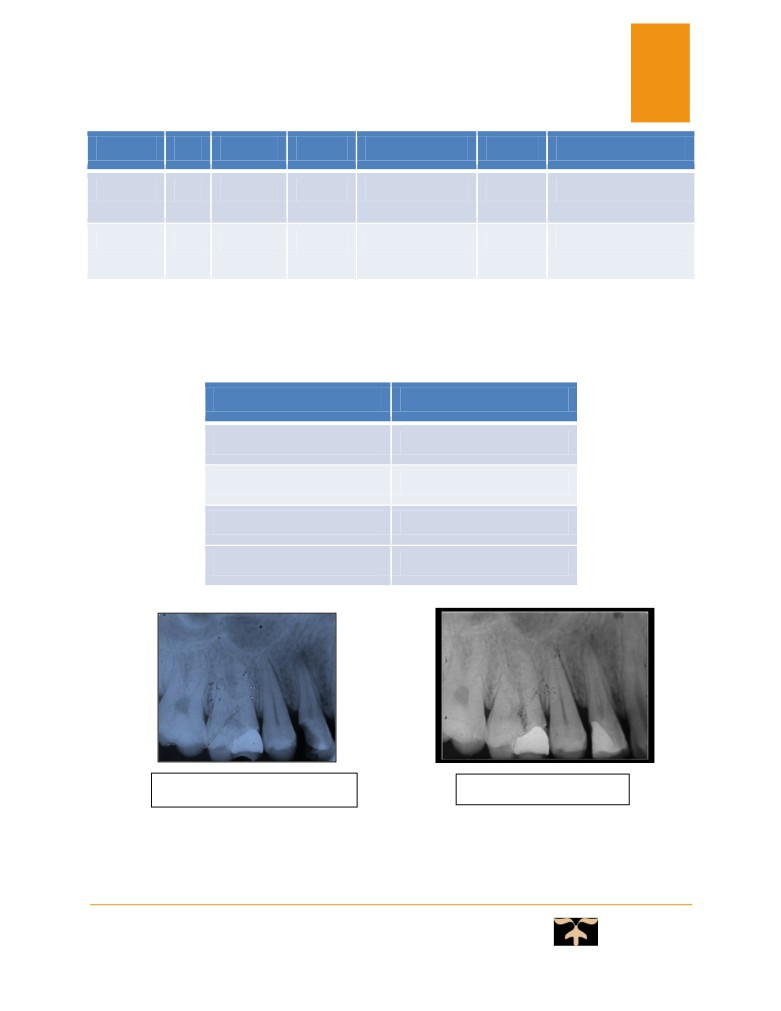
Case 2
Follow up
PAI score
1 month
3
3 months
2
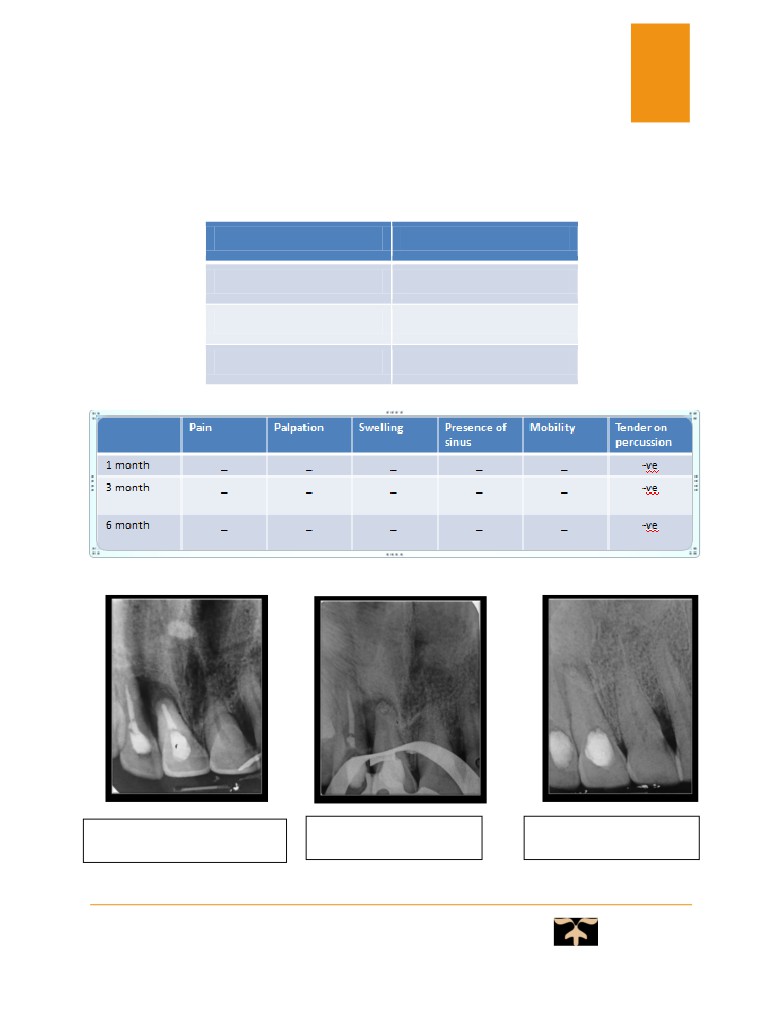
Pre-operative IOPA-R with 21
After 1 month follow up
After 3 months follow up
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
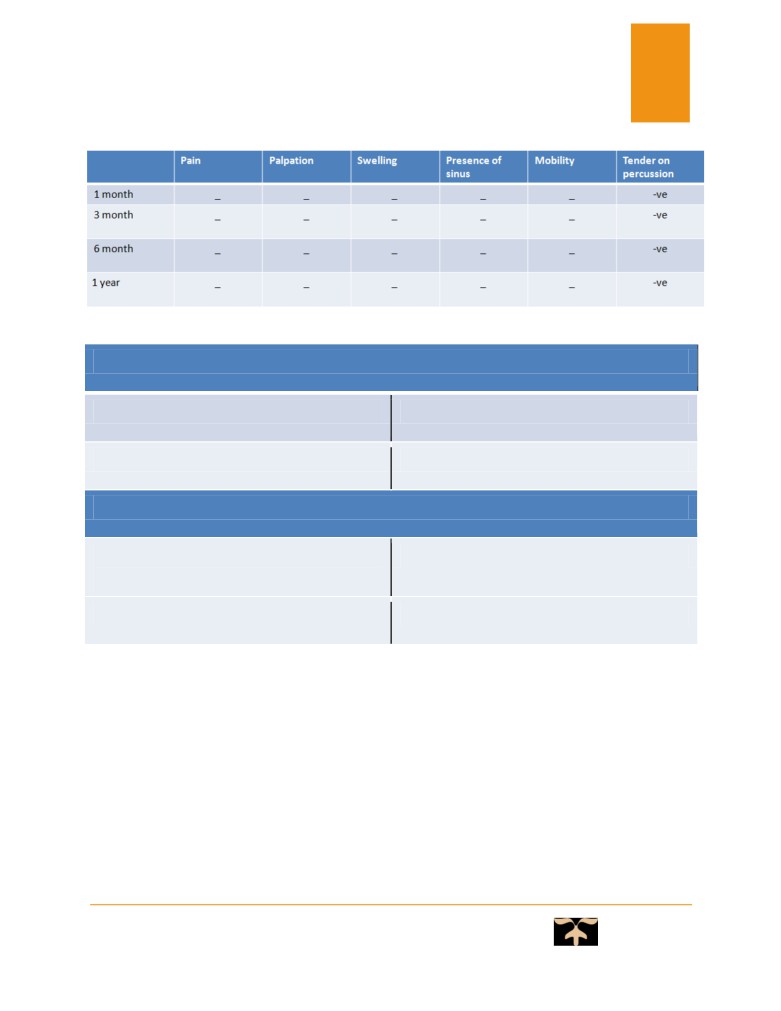
27
Follow up
Pain
Palpation
Swelling
Presence of sinus
Mobility
Tender on percussion
1 month
_
_
_
_
_
-ve
3 month
_
_
_
_
_
-ve
The patient was lost to follow up after 3 months so pulp sensibility tests could not be performed in this case.
Case 3
Follow up
PAI score
1 month
4
3 months
2
6 months
2
1 year
1
Pre operative IOPA-R with 14
After 6 months follow up
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
28
PULP SENSIBILITY TEST
THERMAL (COLD)
Positive response
ELECTRICAL PULP TESTING
Positive response
PULP VITALITY TESTS
PULSE OXIMETRY
72 (normal range=71%-92.7%)7
(OXYGEN SATURATION)
The patient was asymptomatic at the end of 1 year and is still under follow up.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
DISCUSSION
29
Mechanics behind revascularization is that, despite the pulp being necrotic, some pulp tissue along with HERS
(Hertwig’s epithelial root sheath) may survive apically which under favorable conditions proliferate to aid in
the process of regeneration. Case 1was performed following this protocol of induction of bleeding in the canal.
The patient was asymptomatic at the end of six months clinically and there was improvement in the periapical
index score compared to the baseline score. Biological scaffolds have a trimolecular or equilateral fibrin
branch junction which makes its architecture flexible and can support cytokine enmeshment and cellular
proliferation. The tissues inside the root canal appeared to be an extension of the tissues in the periapical area.
Case 2 was lost to follow up at the end of
3 months. The patient was asymptomatic clinically and
radiographically during this period. Animal studies also showed that there was lack of formation of pulp and
dentin like structures with all scaffold types and that the tissue resembled cementum, PDL, bone in majority of
the case (Altaii et al. 2017). Thus, the narrowing of root apex, root lengthening and thickening occurs by
deposition of cementum like and bone like tissue and not dentin. In regenerative endodontic treatment,
cementoblast like cells are derived from progenitor/stem cells in PDL. It is not clear whether these cells enter
the canal immediately after inducing of bleeding or clot formation. The mechanism by which these cells
differentiate into cementoblast like cells is unknown. Second generation platelet concentrates contains and
releases different growth factors that stimulate bone and soft tissue healing. The third case performed was
followed up for a period of 1 year. At the end of six months and 1 year, the oxygen saturation #14 was 72%
which was within the normal range.
CONCLUSION
There may be many ways of looking at a part of problem and developing solution, so the use of blood derived
autologous matrix may be one of those methods to do so which will reduce the need for store of materials and
equipment at the same time paving the way towards customized biological alternatives for treatment.
According to the follow up criteria, case 3 where modified protocol of induction of bleeding followed by
introduction of biological scaffold into the canal space was followed showed better outcome compared to the
other two techniques employed. The cases are under follow up and are showing favorable outcome.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
30
REFERENCES:
1. Murray PE, Garcia Godoy F, Hargreaves KM: Regenerative endodontics: a review of current status and
a call for action, J Endod. 2007. 33: 377.
2. Hermann BW: On the reaction of the dental pulp to vital amputation and calxyl capping.]. Dtsch
Zahnarztl Z. 1952, 7: 1446.
3. Fitzgerald M, Chiego DJ, Jr, Hey DR: Autoradiographic analysis of odontoblast replacement following
pulp exposure in primate teeth. Arch Oral Biol, 1990. 35: 707.
4. Mehta S, Watson JT. Platelet rich concentrate: basic science and current clinical applications. J Orthop
Trauma. 2008;22: 432-8.
5. CARE checklist of information to include when writing a case report, 2013.
6. AAE Clinical Considerations for a Regenerative Procedure Revised 4/1/2018.
7. Kakino S, Kushibiki S. Optical measurement of blood oxygen saturation of dental pulp. ISRN
Biomedical Engineering, 2013; 1-6.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
31
PARTICULARS OF CONTRIBUTORS:
1. Dr. Paromita Mazumdar, Professor and Head, Department of Conservative Dentistry and
Endodontics, Guru Nanak Institute of Dental Sciences and Hospital
2. Dr. Shromi Roy Choudhury, Post Graduate Trainee, Department of Conservative Dentistry and
Endodontics, Guru Nanak Institute of Dental Sciences and Hospital
3. Dr. Sampurna Dutta Gupta, Assistant Professor, Haldia Institute of Dental Sciences and Research
CORRESPONDING AUTHOR:
Name - Dr Shromi Roy Choudhury
Address - Department of Conservative Dentistry and Endodontics, Gurunanak
Institute of Dental Sciences and Research
Contact - 8095739981
E-mail address - shromi.rc2013@gmail.com
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021