Delayed Immediate Denture - A Case Report
Kaustubh Bhapkar 1
Sunil Kumar MV 2
Harikesh P Rao 3
Rajesh Kumar 4
1
Delayed Immediate Denture - A Case Report
ABSTRACT
In today’s world of social activeness, patients demand for an immediate
replacement of missing teeth. Immediate denture is a dental prosthesis constructed
for restoration of tooth immediately after extraction for esthetic as well as
functional reasons. It has been a treatment of choice for cases with trauma,
periodontal disease and various other reasons. Immediate denture acts as a splint
over the surgical area and promotes rapid healing. The purpose of the present
clinical report is to provide the patient with immediate denture. Delayed
immediate denture is given in this case as this was a traumatic case with two teeth
i.e. 21 and 22 avulsed but due to the poor prognosis of 11 made this a delayed
immediate denture case.
KEYWORDS - Avulsion, Denture, Immediate denture.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
2
INTRODUCTION
As documented by Richardson in the year 1860 later discussed by Sears in 1951 and Gehl and
Dresen in 19581 - at various times when some natural teeth are still remaining, dentures are advised to be
constructed before removal of teeth.
According to Glossary of prosthodontic terms 92 - “Immediate denture is any fixed or removable
dental prosthesis fabricated for placement, immediately following the removal of a natural dentition”
Immediate dentures are an important tool for providing patients with an instant replacement
option for extracted teeth. There fabrication is increased nowadays, mainly for aesthetic and
psychological reasons.
CLASSIFICATION
There are: 3
Conventional immediate denture
Interim (or transitional) immediate denture
Conventional immediate denture- one placed after healing is completed and denture is relined to serve
as the long-term prosthesis3.
Interim or Transitional immediate denture- prosthesis is designed to enhance esthetics, stabilization
and or function for a limited period of time, after which it is replaced by a definitive prosthesis3.
The success of immediate dentures depends on correct and precise execution of clinical and laboratory
procedures fulfilling the following requirements:
1. Compatibility with the oral environment.
2. Restoration of masticatory efficiency within limits.
3. Function in harmony with the activity necessary in speech, respiration and deglutition.
4. Aesthetic acceptability.
5. Preservation of remaining hard and soft tissues.4,5
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
3
ADVANTAGES OF IMMEDIATE DENTURE
1. The patient’s psychological and social well-being is preserved.
2. There is less postoperative pain as extraction sites are protected.
3. It acts as a bandage to control hemorrhage.
4. Patient adapts rapidly.
5. It is easier to duplicate natural tooth shape and position.
6. Vertical dimension of occlusion, jaw relationship, and face height can be maintained.
7. Appearance is minimally affected since circum-oral support, muscle tone are maintained.
8. It also helps to preserve the residual ridge with minimum trauma and swelling.
9. It helps the basal tissues, muscles, and joints to acquire a healthy condition.
10. Patient does not develop undesirable habit.6,7
DISADVANTAGES OF IMMEDIATE DENTURES
1. The anterior ridge undercut caused by presence of remaining teeth may interfere with the
impression procedures.
2. Presence of different numbers of remaining teeth in various locations can lead to incorrect
recording of the centric relation position.
3. More chair time, additional appointments are required leading to increased cost.
4. No anterior try in can be done so the esthetics of the denture cannot be evaluated until the
insertion.8
INDICATIONS FOR IMMEDIATE DENTURES
1. Patient who is socially active.
2. Patient who is in good general health.
3. Patient who wish to retain their natural appearance.
4. Patient who is philosophical and understands the scope of treatment modality.
5. Patient who can afford multiple visits.4,6,9
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
4
CONTRAINDICATIONS FOR IMMEDIATE DENTURES
1. Patient who cannot afford time for appointment.
2. Patient who is financially under privileged.
3. Indifferent patients who cannot understand the effort of the dentist for the treatment.
4. Patients with extensive bone loss.
5. Patient who is in debilitated conditions.
6. Systemic conditions which may preclude multiple extractions.
7. Uncooperative and elderly patients.
8. Patients who is emotionally disturbed or diminished mental capacity.
9. Acute periapical or periodontal pathosis. 3,5
CASE REPORT
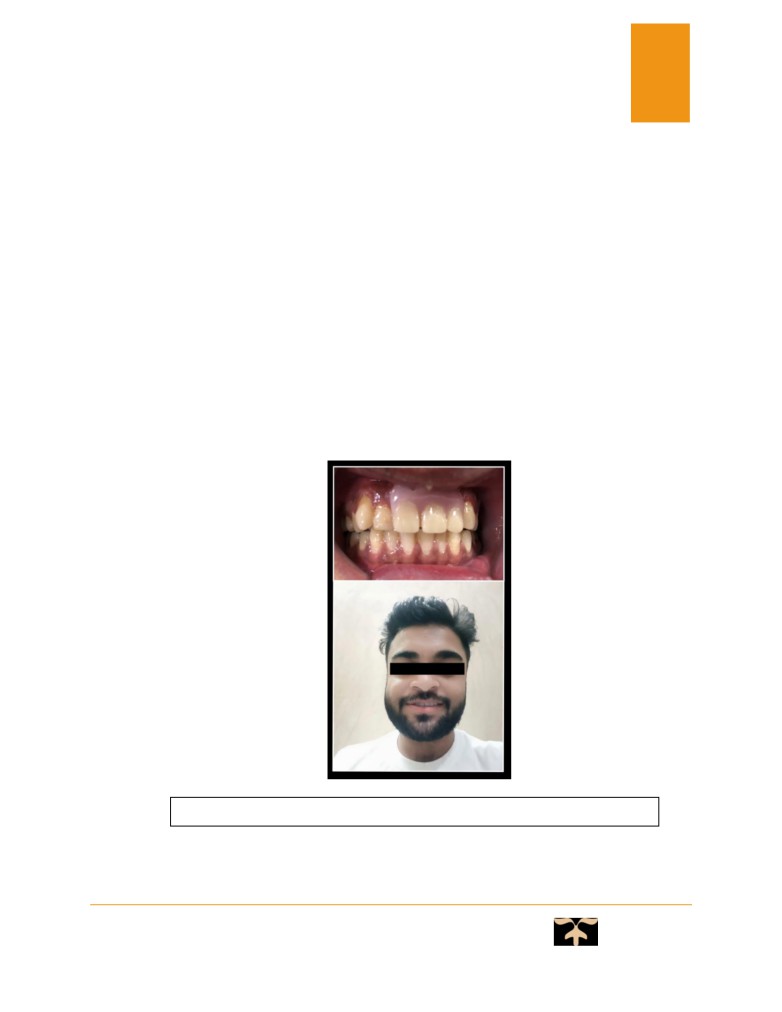
A 20 year old male patient was referred to the Department of Prosthodontics from the department
of Oral Surgery at Jaipur Dental College, who complained of mobility of anterior tooth-11.
His history revealed that the patient met with an accident 1 day before, with avulsion of 21, 22.On
clinical examination, anterior tooth i.e. 11 was found to be grade III mobile, with gingival inflammation.
There was no medical history relevant pertaining to case and no adverse habits. (Fig.1)
Fig. 1 - Preoperative photograph
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
5
Arch size of both maxillary and mandibular ridges were medium in size and arch form of
maxillary and mandibular ridges was square. Ridge form in maxillary ridge was U shaped and mandibular
ridge was inverted U shaped.
Taking into consideration the poor prognosis of tooth, even after a periodontal consideration, a
treatment plan was decided upon to extract the affected tooth, followed by the fabrication of an immediate
partial denture.
Why it is called delayed immediate denture:
As according to the immediate denture definition, when the natural tooth is completely out of
socket or when the natural tooth is extracted an immediate denture has to be placed which we can give it
in relation to 21,22. But in this case 11 is also having poor prognosis and is indicated for extraction, we
have to wait for 11 to get extracted which made this as delayed immediate denture in relation to 21,22 and
an immediate denture for 11.
Investigation before procedure
Lab Investigation: Hb, TLC, DLC, ESR, BT/CT
Radiographs: IOPA
Clinical procedure
Before doing any clinical step the cotton plug which was soaked in Betadine solution and was
inserted into the socket in relation to
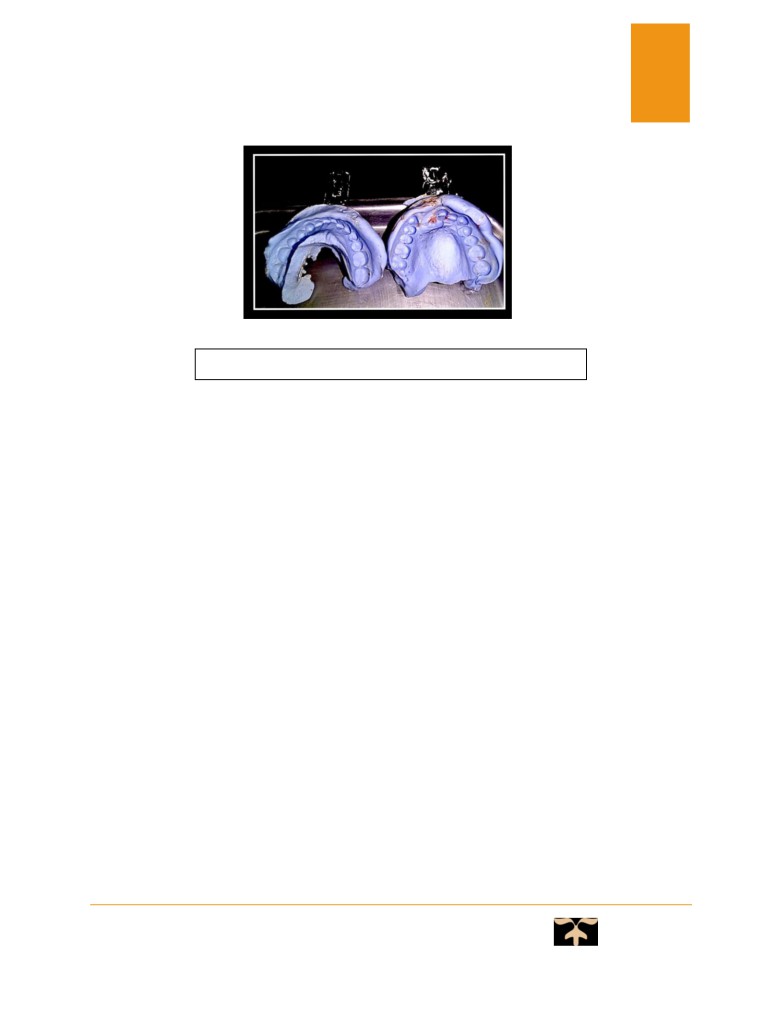
21 and 22.Before extraction, primary upper and lower arch
impression were made with irreversible hydrocolloid impression material i.e., Alginate impression
material in a perforated stock tray. (Fig.2)
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
6
Fig. 2 - Primary impression of upper and lower arch
The teeth selection on the patient has been done under natural light on the same day. Casts were
poured with type III Dental stone. We need to remove the teeth i.e. 11 after making the cast and then
scoring of the cast was done. This step is critical step, as final cast should resemble the alveolar ridge
after complete extraction and healing.
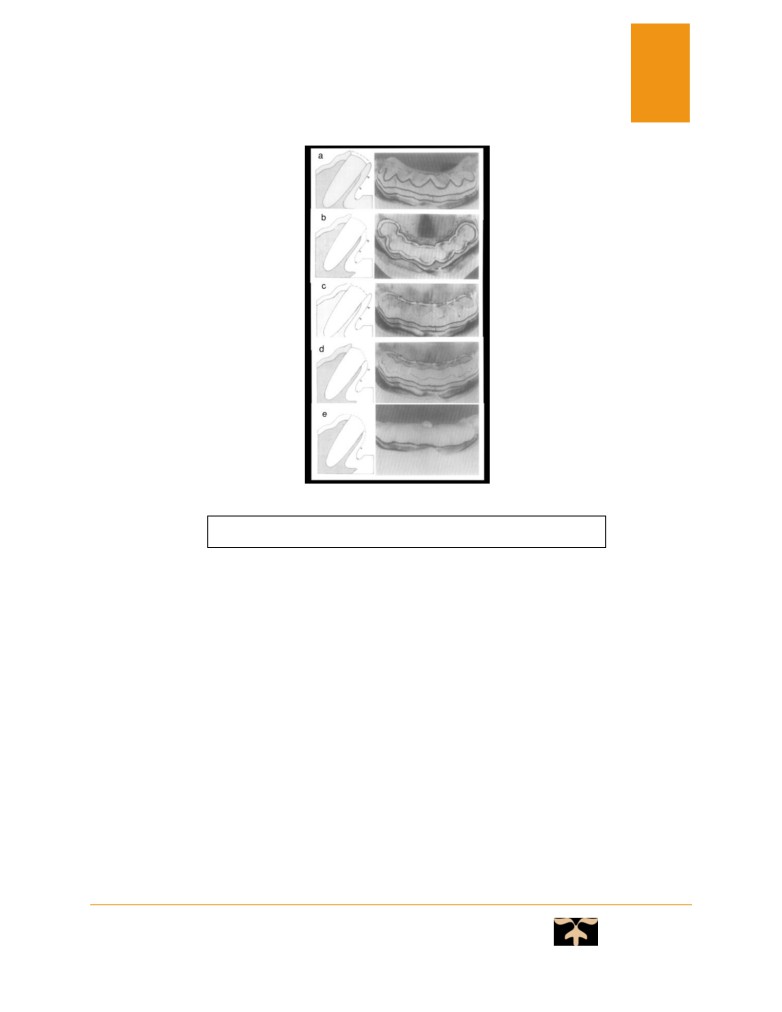
STEPS TO REMOVE THE TOOTH AND SCORING
1. Remove the tooth i.e. 11 at gingival level (Fig.3a)
2. Recess socket by 1mm (Fig.3b)
3. Labial edge recess to incisal third mark (Fig.3c)
4. Mid-point recess to mid-width labial cut (Fig.3d)
5. Round over lingual aspect of the socket (Fig.3e)
6. Round over labial to middle third and sand smooth (Fig.3e) 10
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
7
Fig. 3a-e - Steps to remove the tooth from the cast.
After this the partial record base has been made in relation to 11, 21, 22 followed by occlusal rim
on the cast. These casts were then mounted on a semi adjustable articulator. Then teeth arrangement, wax
up and carving were done, after that the casts are demounted for flasking, dewaxing, packing and curing
of the denture. After completion of acrylization, finishing and polishing of final denture was done.
BEFORE EXTRACTION:
The patient has been informed about all the pros and cons of the procedure and consent form has
been taken.
Prior to surgery, teeth were given prophylaxis for removal of supra and sub-gingival calculus.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
8
EXTRACTION:
Extraction was done under local anesthesia.
Extraction was done by giving nerve block anesthesia not infiltration as it alters the mucosal
topography leading to problem in denture retention.
Extraction was completely atraumatic. (Fig.4)
Fig. 4 - Post-extraction photograph.
AFTER EXTRACTION:
Once the bleeding stopped, insertion of the cured denture was done. Denture was inserted after 30
minutes of extraction for allowing the clot to stabilize.
It was made sure that the socket was filled with blood before inserting the denture.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
9
POST OPERATIVE INSTRUCTION:
The patient was asked to wear the denture for 24 hours without removing.
The patient was asked to prevent vigorous mouth washing.
The patient was informed to avoid smoking, alcohol, hot food and drink to reduce possibility of
post extraction hemorrhage.
Analgesics and antibiotics were prescribed for 3 days BD.
Patient was asked to report after 24 hours, to check for any ulcer formation and also to check the
healing. Surgical area was irrigated with saline and betadine.
After 48 hours, the denture was relined with a temporary soft liner, so that no ulceration of the
soft tissue due to denture occurs. The patient was recalled after 1week, 3 weeks, 2 months and 4 months
on follow up. (Fig.5).
Fig 5- Post-operative view of a happy patient.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
10
CONCLUSION
Immediate complete denture treatment should still be considered as an important
treatment modality, in the era of implant and immediate implant treatment.
Treatment planning must be flexible. A variety of workable techniques is available, but
the one that best fits the unique requirements of the patient should be selected.
The alveolar bone must be conserved. It is best to perform little or no alveoloplasty on
removal of the anterior teeth. The dentist must be aware of the emotional needs of his
patient. Psychological factors are extremely important. Neglect in this area can result in
failure in terms of overall patient satisfaction, in spite of the finest treatment planning and
technical expertise.
The immediate denture must be considered as one part of overall treatment. There is no
such thing as a permanent denture. The immediate denture is one part of what must be a
continuing, ongoing professional service. The patient must be educated accordingly.
Periodic recall, examination, rebasing, and adjustments are imperative for optimal health
care.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
11
REFERENCES:
1. Gehl, D.H., and Dresen, O.M. Complete denture prosthesis, ed 4. Philadelphia, W. B.
Saunders Co., 1958, p 424.
2. Glossary of Prosthodontic terms- 9: e47
3. Zarb GA, Bolender CL. Prosthodontic treatment for edentulous patients, 12th ed, 2009, St.
Louis, Mosby, 123-59.
4. Lavere A.M, Krol A.J. Immediate denture service. J Prosthet Dent. 1973;29:10-5.
5. Heartwell, C. and Salisbury, F. W. Immediate complete dentures: An evaluation. J Prosthet
Dent 15:615-624, 1965.
6. MV Kumar Sunil et al. immediate dentures - A case report. Journal of clinical dentistry.
2011: 43-50.
7. Kadam Ishan et al. restoring smiles with conventional immediate denture: a case report.
International Journal of Recent Scientific Research. 2018;9(6):27503-27508.
8. Vinay Pavan Kumar Kadavakolanu et al. Fabricaction of immediate interim complete
dentures using modified Poly vinyl siloxane sectional impression technique: A Case Report.
International Dental Journal of Student Research; June 2016;4(2):87-93.
9. Payne, S. H. A transitional denture. J Prosthet Dent 14:221-230, 1964.
10. Jerbi FC. Trimming the cast in the construction of immediate dentures. J Prosthet Dent.
1966;16: 1047-53.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
12
PARTICULARS OF CONTRIBUTORS:
1. Dr. Kaustubh Bhapkar, Postgraduate student, Jaipur Dental College, Jaipur.
2. Dr. Sunil Kumar MV, MDS, Professor and PG Director, Jaipur Dental College, Jaipur.
3. Dr. Harikesh P. Rao, MDS, Professor and HOD, Jaipur Dental College, Jaipur.
4. Dr. Rajesh Kumar, MDS, Professor, Jaipur Dental College, Jaipur.
DEPARTMENT AND INSTITUTION:
Department of Prosthodontics, Crown and Bridge and oral Implantology, Jaipur Dental College, Jaipur,
Rajasthan, India
CORRESPONDING AUTHOR:
Name - Dr. Kaustubh Bhapkar
Address - 85, Anurag Nagar, Part-2, Indore, Madhya Pradesh, 452010.
Contact - 7748888869
E-mail address - kaustubh.bhapkar25@gmail.com
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021