Resin Infiltration Technique To Treat
Hypomineralized Incisors - A Case Report
Dr. Aindrila Ghosh 1
Dr. Paridhee Jalan 2
Dr. Aaheli Banerjee 3
Prof. (Dr.) Shabnam Zahir 4
Dr. Sudipta Kar 5
Prof. (Dr.) Gautam Kundu 6
13
Resin Infiltration Technique to Treat
Hypomineralized Incisors - A Case Report
ABSTRACT
Molar incisor hypomineralization (MIH) is a commonly occurring developmental
defect causing esthetic concerns among most patients. Depending upon the severity
of the lesion various treatment options are available like bleaching, microabrasion,
resin infiltration, composite resin bonding or a combination of all the techniques.
This case report highlights the use of resin infiltration (ICON) in the treatment of
hypomineralized incisors. The resin penetrates the lesion microporosities by
capillary force and is hardened by curing with light. The infiltrated enamel has a
similar appearance to that of sound enamel. Moreover it also arrests the further
progression of lesion. This technique is gaining importance with passing years
because it not only provides esthetic rehabilitation but also allows recovery from
hypomineralization.
KEYWORDS - Molar incisor hypomineralization, white spot, resin infiltration, ICON, recovery.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
14
INTRODUCTION
Molar incisor hypomineralisation is a developmentally derived dental defect that involves hypomineralisation
of one to four first permanent molars and frequently associated with similarly affected permanent incisors.
According to Weerheijm et al (2001)1, its defined as ‘hypomineralisation of systemic origin , presenting as
demarcated , qualitative defects of enamel of one to four first permanent molars frequently associated with
affected incisors’. White spot lesions are early signs of demineralization which may result in development of
caries. These lesions may cause esthetic concerns among patients due to enamel discoloration and also
increases the susceptibility of the tooth to fracture due to reduction in the inorganic component of enamel 2. The
treatment of these lesions aims both at improving esthetics as well as prevention of caries progression.
Worldwide the prevalence ranges from 2.4% to 40.2% 3. Study conducted in Delhi in the year 2019 showed
prevalence rate of 1.17% in children of age group 6-12 years and the severity in incisors was 24.24%and that of
molars was 52.27% 4.No gender difference has been noted in multiple studies.
CASE REPORT
A 7 years old male patient, reported to the Outpatient department of Pediatric and Preventive dentistry of
Guru Nanak Institute of Dental Sciences and Research, with the chief complaint of brown spots in upper
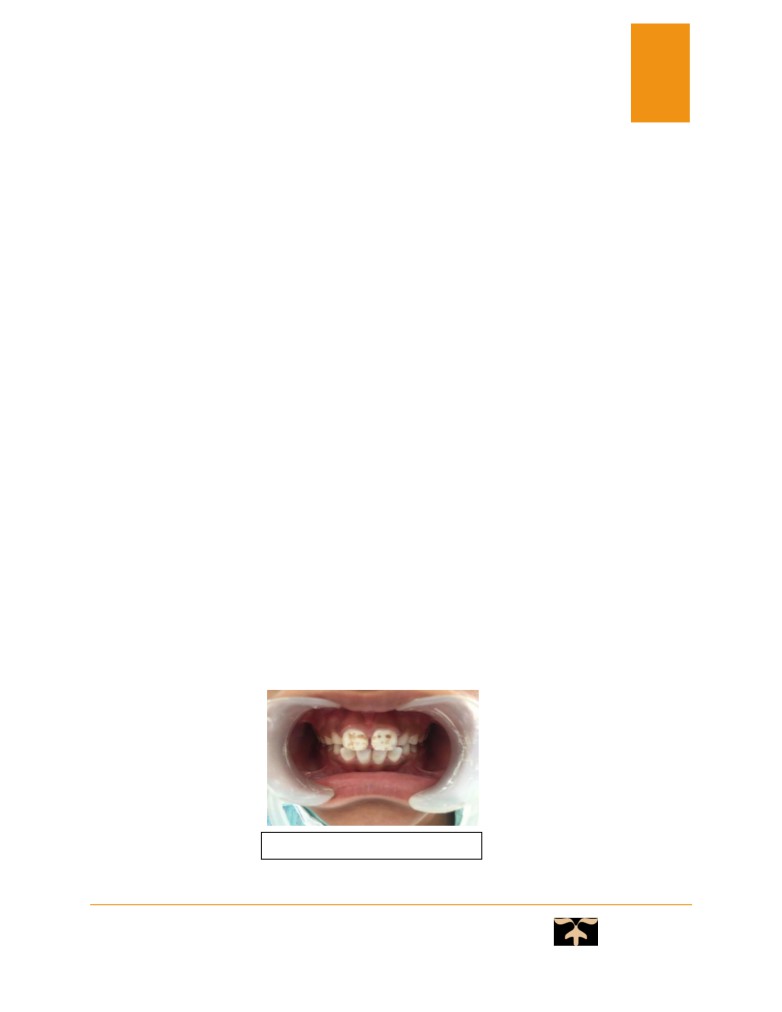
front teeth region for last few years. The medical history was irrelevant. On clinical examination chalky
white opacities and brownish grooves of different depth and diameter were noted on the entire labial
surface of 11 and 21 (Fig 1). Similar opacities were also noted on 16 and 26.The treatment plan for this
case was:
•
Resin infiltration technique using “icon” for chalky white opacities.
•
Flowable composite to restore the brownish pits, fissures and grooves.
Fig. 1 - Pre-operative view
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
15
PROCEDURE
The following clinical steps were conducted:
Oral prophylaxis of the affected teeth using a non-fluoridated prophylactic paste followed by isolation of
affected teeth using rubber dam so as to obtain a clean dry field and protect the soft tissues (Fig 2).
The surface of white spot was eroded by application of icon etch containing 15% hydrochloric acid using a
microbrush, for 2 minutes 5 to create microporosities within the enamel (Fig 4) . It also removes superficial
discoloration and the higher mineralized surface layer that may hamper the penetration of resin. The etchant is
then washed subsequently for 30 seconds followed by application of icon dry containing ethanol to desiccate
the lesion (Fig 5) .The icon infiltrant containing TEGDMA, is then applied using a microbrush over the lesion
and is allowed to penetrate for 5 minutes6,7(Fig 6). The excess is then removed with a cotton pellet and light
cured (Fig 7).The application of infiltrant is repeated 2 to 3 times to reduce enamel porosities. Flowable
composite is applied over the icon infiltrant followed by light curing (Fig 8,9) .Finally the rough surface is
polished with rubber disks 6 to obtain a smooth surface (Fig 10) and post-operative instructions were given to
the patient.
Fig. 2 - Isolation
Fig. 3 - Icon Kit
Fig. 4 - Etching
Fig 5- Icon Dry Application
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
16
DISCUSSION
Icon infiltrant contain TEGDMA which produces better inhibition of hypomineralized lesion progression than
BISGMA (in conventional bonding agents) due to better penetration capabilities after ethanol application 7.
Icon etch contain 15% hydrochloric acid gel which creates more microporosities than that with 37%
orthophosphoric acid thereby increasing penetration capability of “icon”8,9.
The refractive index of icon infiltrant is 1.46 ,which is very similar to that of enamel (1.62) thereby after its
application the chalky white lesion appears similar to that of sound enamel 10.
Resin infiltration technique is a microinvasive cosmetic technique that fills, reinforce, masks and stabilize
demineralized enamel, improving esthetics, preventing caries progression , sensitivity and increasingthe patient
compliance in cases with mild MIH.
But in cases of severe MIH, resin infiltration technique alone is not enough to mask the enamel defect and
requires the use of composite resin restoration along with it.
CONCLUSION
The early diagnosis and treatment of MIH is crucial as more porous enamel disintegrates more easily, not to
underestimate the esthetic considerations, thereby psychological effects on the child with MIH.Thus with
time the demand of resin infiltration technique are soaring high as it not only provides esthetic rehabilitation
but also allows recovery from hypomineralization.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
17
REFERENCES:
1.
Weerheijm K L, Jalevik B, Alaluusua S. Molar-incisor hypomineralisation. Caries Res .2001;
35:390-391.
2.
Weerheijm K L, Duggal M, Mejare I et al. Judgement criteria for molar incisor
hypomineralisation (MIH) in epi¬demiologic studies: a summary of the European meeting on
MIH held in Athens, 2003. Eur J Paediatr Dent. 2003; 4:110-113.
3.
Ghanim A, Silva M J, Elfrink M E C et al. Molar incisor hypomineralisation (MIH) training
manual for clinical field surveys and practice. Eur Arch PaediatrDent . 2017; 18:225-242.
4.
Goswami M, BhushanU,et al. Molar Incisor Hypomineralization - An Emerging Burden. A
Short Study on Prevalence and Clinical Characteristics in Central Delhi, India. Int J Clin Pediatr
Dent.2019;12 (3): 211-214.
5.
Paris S, Meyer-Lueckel H. Inhibition of caries progression by Resin infiltration in situ. Caries
Res. 2010; 44: 47-54.
6.
Paris S, Meyer-Lueckel H. Masking of labial enamel white spot lesions by resin infiltration -a
Clinical report. Quintessence Int. 2009; 40:713-8.
7.
Meyer-Lueckel H, Paris S. Progression of artificial enamel caries lesions after infiltration with
experimental light curing resins. Caries Res. 2008;42:117-24.
8.
Paris S, Meyer-Lueckel H, KielbessaAM. Resin infiltration of natural caries lesion. J Dent Res.
2007;86:662-6.
9.
Meyer-Lueckel H, Paris S, Kielbassa AM. Surface layer erosion of natural caries lesion with
phosphoric and hydrochloric acid gels in preparation for resin infiltration. Caries Res. 2007; 41:
223-30.
10. Manoharan V, Kumar AS,et al. Is Resin Infiltration a Microinvasive Approach to White Lesions
of calcified tooth structure? A Systemic Review. Int J ClinPediatrDent.2019; 12(1): 53-58.
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021
18
PARTICULARS OF CONTRIBUTORS:
1. Dr. Aindrila Ghosh, Post Graduate Student. Department of Pediatric and Preventive Dentistry,
Guru Nanak Institute of Dental Sciences and Research. 157/F Nilgunj Road, Panihati, Kolkata -
700114
2. Dr. Paridhee Jalan, BDS, MDS. Department of Pediatric and Preventive Dentistry, Guru Nanak
Institute of Dental Sciences and Research. 157/F Nilgunj Road, Panihati, Kolkata -700114
3. Dr. Aaheli Banerjee, Post Graduate Student. Department of Pediatric and Preventive Dentistry,
Guru Nanak Institute of Dental Sciences and Research. 157/F Nilgunj Road, Panihati, Kolkata -
700114
4. Prof. (Dr.) Shabnam Zahir. BDS, MDS. Professor, Department of Pediatric and Preventive
Dentistry, Guru Nanak Institute Of Dental Sciences and Research.157/F Nilgunj Road, Panihati,
Kolkata -700114.
5. Dr. Sudipta Kar, BDS, MDS. Reader, Department of Pediatric and Preventive Dentistry, Guru
Nanak Institute of Dental Sciences and Research. 157/F Nilgunj Road, Panihati, Kolkata -700114
6. Prof.
(Dr.) Gautam Kundu. MDS. Professor and Head of the Department, Department of Pediatric
and Preventive Dentistry, Guru Nanak Institute of Dental Sciences and Research. 157/F Nilgunj
Road, Panihati, Kolkata -700114.
DEPARTMENT AND INSTITUTION:
Department of Pediatric and Preventive Dentistry, Guru Nanak Institute of Dental Sciences and Research.
157/F Nilgunj Road, Panihati, Kolkata -700114
CORRESPONDING AUTHOR:
Name - Dr. Aindrila ghosh
Contact - 9674187424
E-mail address - ghosh.aindrila699@gmail.com
The Chronicles Of Stomatology Vol.1 Issue 1 Jan-Mar, 2021